There is a myth among prosecutors, defense attorneys and judges that is propagated time and again all over courtrooms in the US that involves the idea of “therapeutic ranges” when it comes to DUID cases and prescribed drugs. The notion is that there is a one-size fits all chart that we can all refer to in order to settle the question of whether or not there is impairment based upon a drug in a given case. I understand why that is so attractive to prosecutors, judges and defense attorneys because it is a shortcut to thinking. It saves time. However, scientifically, there is no such thing.
I call it “cookie cutter pharmacology.” It is dangerous for traffic safety. It is dangerous to justice. It is just plain dangerous.

Can anyone use the “cookie cutter” charts such as Winek’s, Basselt’s and the like to his or her advantage in pre-trial discussions with opposing counsel to try to attain some sort of favorable result? Sure. Absolutely. In fact, it is done every single day. But is it right? No. Here’s why.

Do not try to use these charts against someone who even marginally educated in the pharmacology. Reliance on such charts is not scientifically warranted for many reasons:
- These charts were developed for postmortem use in autopsy cases as a guide to help determine cause of death from an overdose as a potential cause of death, not impairment for a driver. It is a guide or resource for further investigation in postmortem toxicology – that is all.
- There are no footnotes as to the sources of the literature for the published levels. If you pull the original research you will find some that will differ significantly.
- All you have to do is to look at the 2001 Winek’s Drug & Chemical Blood-Level Data chart to see several items that are the same thing listed independently based upon their generic name versus a trade name, but have different reported values. For example: Ambien and Zolpidem. Ambien is the trade name and Zolpidem is the drug. Both are the same darn thing, but when looking at the chart we see:
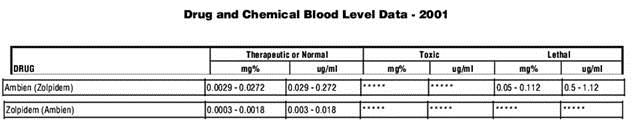
It does not make sense.
- The matrix and the measurand are not reported in the reported values. Some are plasma results, some whole blood, and some are urine. There is a large difference among them. What is your lab report?
- What is the time of collection versus time of last driving of your case versus what was here in the chart? This is massively relevant.
- The simple fact is that someone who is using an acute dose and is pharmacologically naive to the drug can absolutely be impaired for the purposes of safe driving at a concentration under what is published in these charts.

The true questions in any given DUID impairment case are as follows:
- What is the testifying witness’s definition of “impairment”? Is it to the slightest degree or substantial impairment or something in-between?
- For what purpose is this person’s definition of impairment being used for? For safe driving? For doing roadsides? What?
- Do they have epidemiological or actual driving studies that show odds ratios and crash data or standard deviation of lateral position or follow distance data that support their call that the drug in any amount is even associated with the possibility of a crash?
- Can the observations of the officer at roadside be linked uniquely to the results of a blood test at time of blood draw which is far removed from the time of actual driving? What is the pharmacokinetic behavior of the drug? We never get the blood draw at the time of driving and no one can legitimately use retrograde extrapolation to get to the drug level at the time of driving and observation. You cannot tell where one is on the pharmacokinetic cycle based upon a single blood draw point.
- How much stock does the opining expert who makes the impairment call place in the unverified observations of the police officer? Or is there objective information such as video? Consider the case of amphetamines alone (no ethanol). If you add this equation the published information that if a DRE officer (the highest trained officer per NHTSA using the most complex series of testing done by officers) was present and did the full battery of the DRE evaluation, then that most highly trained officer using the DRE diagnostic tool only has a likelihood ratio of .083 (which is a negative correlation) in correctly predicting amphetamine PRESENCE in the person’s system, and that in one peer reviewed study that the accuracy rate for stimulants presence IN URINE (amphetamine is a stimulant) was only 9%, then how on earth can your minimally trained Academy-only educated officer stand a snowball’s chance in Hades to correctly opine presence…. let alone impairment due to this drug using far less to investigate and knowing far less? None I assert.
- How much (or little) does the opinion expert know about that human being who they are making this important judgment about?
So in conclusion, if you are confused after reading all of this, you are right to be confused. Mama is right, we are all beautiful snowflakes. For DUID impairment cases “Life is like a box of chocolates. You never know what you are going to get” when it comes to evaluating a stranger and having no meaningful pharmacological data or history.
Well trained forensic scientists who understand pharmacology are rare. Exceedingly rare. We all want a just result. We all want safe roads. We want the innocent driver who is following doctor’s orders and is not impaired not to go to jail and lose his or her driver’s license. We all want dangerous impaired drivers off the road. In sum, we all want to get it right.
This is why we have to educate ourselves on the value of “cookie cutter” pharmacology and avoid it. Justice demands no less.

 The McShane Firm | DUI Lawyers
The McShane Firm | DUI Lawyers Pennsylvania DUI Blog
Pennsylvania DUI Blog